In 1993, Ian Stevenson MD, head of the Department of Psychiatric Medicine
at the University of Virginia School of Medicine located in Charlottesville,
Virginia, published the article reproduced below. It later was the basis for
the book
"Where Reincarnation and Biology Intersect"
pictured).
Entitled
"Birthmarks and Birth Defects
Corresponding to Wounds on Deceased Persons",
this article was based on his presentation at the Eleventh Annual Meeting
of the Society for Scientific Exploration at Princeton University in June 1992.
Why Reincarnation and Biology Intersect
This is dramatic evidence of how past life traumas become so embedded in
an individual's
cellular memory
that they are carried from one life to the next.
Now Dr. Stevenson Speaks for Himself
About His Research
ABSTRACT:
Almost nothing is known about why pigmented birthmarks
(moles or nevi) occur in particular locations of the skin. The causes of
most birth defects are also unknown. About 35% of children who claim to
remember previous lives have birthmarks and/or birth defects that they (or
adult informants) attribute to wounds on a person whose life the child
remembers. The cases of 210 such children have been investigated.
The birthmarks were usually areas of hairless, puckered skin; some were
areas of little or no pigmentation (hypopigmented macules); others were
areas of increased pigmentation (hyperpigmented nevi). The birth defects
were nearly always of rare types.
In cases in which a deceased
person was identified the details of whose life unmistakably matched the
child's statements, a close correspondence was nearly always found between the
birthmarks and/or birth defects on the child and the wounds on the
deceased person.
In 43 of 49 cases in which a medical
document (usually a postmortem report) was obtained, it confirmed the
correspondence between wounds: and birthmarks (or birth defects). There
is little evidence that parents and other informants imposed a false
identity on the child in order to explain the child's birthmark or birth
defect.
Some paranormal process seems required to account for
at least some of the details of these cases, including the birthmarks
and birth defects.
Figure 1
Hypopigmented macule on chest of an Indian
youth who, as a child, said he remembered the life of a man, Maha Ram,
who was killed with a shotgun fired at close range.
Figure 2
The circles show the principal shotgun wounds on
Maha Ram, for comparison with Figure 1.
[This drawing is from the autopsy report of the deceased.]
INTRODUCTION:
Although counts of moles (hyperpigmented nevi)
have shown that the average adult has between 15 and IX of them (Pack and
Davis,1956), little is known about their cause -- except for those associated
with the genetic disease neurofibromatosis -- and even less is known about
why birthmarks occur in one location of the body instead of in another.
In a few instances a genetic factor has been plausibly suggested for the
location of nevi (Cockayne, 1933; Denaro, 1944; Maruri, 1961);
but the cause of the location of most birthmarks
remains unknown.
The causes of many, perhaps most, birth defects remain similarly
unknown.
In large series of birth defects in which investigators
have searched for the known causes, such as chemical teratogens (like
thalidomide), viral infections, and genetic factors, between 430/0
(Nelson and Holmes, 1989) and 65 -- 70% (Wilson, 1973) of cases have
finally been assigned to the category of "unknown causes."
Among 895 cases of children who claimed to remember a previous life (or
were thought by adults to have had a previous life), birthmarks and/or
birth defects attributed to the previous life were reported in 309 (35%)
of the subjects.
The birthmark or birth defect of the child
was said to correspond to a wound (usually fatal) or other mark on the
deceased person whose life the child said it remembered.
This paper reports an inquiry into the validity
of such claims.
With my
associates I have now carried the investigation of 210 such cases to a
stage where I can report their details in a forthcoming book (Stevenson,
forthcoming
(book above -EM).
This article summarizes our findings.
Children who claim to remember previous lives have been found in every
part of the world where they have been looked for (Stevenson, 1983; 1987),
but they are found most easily in South Asia.
Typically, such a child begins to speak about a previous life almost as
soon as it can speak, usually between the ages of two and three; and
it stops doing so between the ages of five and seven
(Cook, Pasricha, Samararatne, Win Maung, and Stevenson, 1983).
Although some of the children make only vague statements,
others give details of names and events that
permit identifying a person whose life and death corresponds to the
child's statements. In some instances
the person identified is already known to the child's
family, but in many cases this is not so. In addition to making
verifiable statements about a deceased person,
many of the children show behavior (such as a
phobia) that is unusual in their family but found to correspond to
behavior shown by the deceased person concerned or conjecturable for
him (Stevenson, 1987;1990).
Although some of the birthmarks occurring on these children are
"ordinary" hyperpigmented nevi (moles) of which every adult has some
(Pack and Davis, 1956), most are not. Instead, they are more likely to
be puckered and scarlike, sometimes depressed a little below the
surrounding skin, areas of hairlessness, areas of markedly diminished
pigmentation (hypopigmented macules), or port-wine stains (nevipammri).
When a relevant birthmark is a hyperpigmented nevus, it is nearly always
larger in area than the "ordinary" hyperpigmented nevus. Similarly, the
birth defects in these cases are of unusual types and rarely correspond to
any of the "recognizable patterns of human malformation" (Smith, 1982).
METHODS:
My investigations of these cases included interviews,
often repeated, with the subject and with several or many other informants
for both families. With rare exceptions, only firsthand informants were
interviewed. All pertinent written records that existed, particularly
death certificates and postmortem reports, were sought and examined. In
the cases in which the informants said that the two families had no
previous acquaintance, I made every effort to exclude all possibility that
some information might nevertheless have passed normally to the child,
perhaps through a half-forgotten mutual acquaintance of the two families.
I have published elsewhere full details about methods (Stevenson, 1975; 1987).
I did not accept any indicated mark as a birthmark unless
a firsthand witness assured me that it had been noticed immediately after
the child's birth or, at most, within a few weeks. I enquired about the
occurrence of similar birth marks in other members of the family; in
nearly every instance this was denied, but in seven cases a genetic factor
could not be excluded.
Birth defects of the kind in question here
would be noticed immediately after the child's birth.
Inquiries in these cases excluded (again
with rare exceptions) the known causes of birth defects, such as
close biological relationship of the parents (consanguinity),
viral infections in the subject's mother during her pregnancy, and
chemical causes of birth defects like alcohol.
RESULTS:
Correspondences between Wounds and
Birthmarks
A correspondence between birthmark and wound was judged satisfactory
if the birthmark and wound were both within an area of 10 square
centimeters at the same anatomical location;
in fact, many of the birthmarks and wounds
were much closer to the same location than this.
A medical document, usually a postmortem report, was
obtained in 49 cases. The correspondence between wound and birthmark
was judged satisfactory or better by the mentioned criterion in 43 (88%)
of these cases and not satisfactory in 6 cases.
Several different
explanations seem to be required to account for the discrepant cases,
and I discuss these elsewhere (Stevenson, forthcoming). Figure 1 shows a
birthmark (area of hypopigmentation) on an Indian child who said he
remembered the life of a man who had been killed with a shotgun fired
at close range. Figure 2 shows the location of the wounds recorded by
the pathologist. (The circles were drawn by an Indian physician who
studied the postmortem report with me.)
The
high proportion (88%) of concordance between wounds and
birthmarks in the cases for which we obtained postmortem reports (or
other confirming documents)
increases confidence in the accuracy of
informants' memories concerning the wounds on the deceased person in
those more numerous cases for which we could obtain no medical document.
Not all errors of informants memories would have resulted in attributing
a correspondence between birth marks and wounds that did nor exist;
in four cases (possibly five) reliance on an informant's memory would
have resulted in missing a correspondence to which a medical document attested.
Figure 3
Large verrucous epidermal nevus on head of a Thai
man who as a child said he remembered the life of his paternal uncle,
who was killed with a blow on the head from a heavy knife.
Cases with Two or More
Birthmarks
The argument of chance as accounting for the correspondence
between birthmarks and wounds becomes much reduced when the child has
two or more birthmarks each corresponding to a wound on the deceased
person whose life he claims to remember. Figure 3 shows
a major abnormality of the skin (verrucous epidermal nevus) on the back
of the head of a Thai man who, as a child, recalled the life of his uncle,
who had been struck on the head with a heavy knife and killed almost
instantly. The subject also had a deformed toenail of the right great
toe (Figure 4). This corresponded to a chronic infection of the same
toe from which the subject's uncle had suffered for some years before he died.
Figure 4
Congenital malformation of nail on right great
toe of the Thai subject shown in Figure 3.
This malformation corresponded
to a chronic ulcer of the right great toe from which the subject's uncle
had suffered.
The series includes 18 cases in which two birthmarks on a subject
corresponded to gunshot wounds of entry and exit. In 14 of these one
birthmark was larger than the other, and in 9 of these 14 the evidence
clearly showed that the smaller birthmark (usually round) corresponded
to the wound of entry and the larger one (usually irregular in shape)
corresponded to the wound of exit. These observations accord with the
fact that bullet wounds of exit are nearly always larger than wounds
of entry (Fatteh, 1976; Gordon and Shapiro, 1982).
Figure 5 shows
a small round birthmark on the back of the head of a Thai boy, and
Figure 6 shows a larger, irregularly shaped birthmark at the front of
his head. The boy said that he remembered the life of a man who was shot
in the head from behind. (The mode of death was verified, but no medical
document was obtainable.) In addition to the 9 cases I have investigated
myself, Mills reported another case having the feature of a small round
birthmark (corresponding to the wound of entry) and a larger birthmark
corresponding to the wound of exit (both verified by a postmortem report)
(Mills, 1989).
Figure 5
Small, round puckered birthmark
on a Thai boy that corresponded to the bullet wound of entry in a man
whose life he said he remembered and who had been shot with a rifle
from behind.
Figure 6
Larger, irregularly shaped birthmark
on the frontal area of the head of the Thai boy shown in Figure 5. This
birthmark corresponded to the bullet wound of exit on the Thai man whose
life the boy said he remembered.
[No Figure 7 - EM]
I have calculated the odds against chance of two birthmarks correctly
corresponding to two wounds. The surface area of the skin of the average
adult male is 1.6 meters (Spalteholz, 1943). If we were to imagine this
area square and spread on a flat surface, its dimensions would be approximately
127 centimeters by 127 centimeters. Into this area would fit approximately
160 squares of the size 10 centimeters square that I mentioned above.
The probability that a single birthmark on a person
would correspond in location to a wound within the area of any of the
160 smaller squares is only 1/160.
However, the probability
of correspondences between two birthmarks and two wounds would be (1/160)2
i.e. 1 in 25,600. (This calculation assumes that birthmarks are uniformly
distributed over all regions of the skin. This is incorrect [Pack, Lenson,
and Gerber, 1952], but I believe the variation can be ignored for the
present purpose.)
Examples of Other Correspondences
between Wounds and Birthmarks
A Thai woman had three separate linear hypopigmented scarlike birthmarks
near the midline of her back; as a child she had remembered the life of a
woman who was killed when struck three times in the back with an ax.
(Informants verified this mode of death, but no medical record was obtainable.)
A woman of Burma was born with two perfectly round birthmarks in
her left chest; they slightly overlapped, and one was about half the size
of the other. As a child she said she remembered the life of a woman who
was accidentally shot and killed with a shotgun. A responsible informant
said the shotgun cartridge had contained shot of two different sizes. (No
medical record was obtainable in this case.)
Another Burmese child said that she remembered the life of her
deceased aunt, who had died during surgery for congenital heart disease.
This child had a long, vertical linear hypopigmented birthmark close to
the midline of her lower chest and upper abdomen; this birthmark corresponded
to the surgical incision for the repair of the aunt's heart. (I obtained
a medical record in this case.)
In contrast, a child of Turkey had a horizontal linear birthmark
across the right upper quadrant of his abdomen. It resembled the scar of
a surgeon's transverse abdominal incision. The child said that he remembered
the life of his paternal grandfather, who had become jaundiced and was
operated on before he died. He may have had a cancer of the head of the
pancreas, but I could not learn a precise medical diagnosis.
Two Burmese subjects remembered as children the lives of
persons who had died after being bitten by venomous snakes, and the
birthmarks of each corresponded to therapeutic incisions made at the sites
of the snakebites on the persons whose lives they remembered.
Another Burmese subject also said as a child that she remembered
the life of a child who had been bitten on the foot by a snake and died.
In this case, however, the child's uncle had applied a burning cheroot
to the site of the bite -- a folk remedy for snakebite in parts of Burma;
and the subject's birthmark was round and located at the site on the foot
where the bitten child's uncle had applied the cheroot.
Three Examples of Birth
Defects
Figure 8, below, shows the right side of the head of a Turkish boy
with a diminished and malformed ear (unilateral microtia). He also had
underdevelopment of the right side of his face (hemifacial microsomia).
He said that he remembered the life of a man who had been shot (with a
shotgun) at point-blank range. The wounded man was taken to a hospital
where he died 6 days later -- of injuries to the brain caused by shot
that had penetrated the right side of the skull. (I obtained a copy of
the hospital record.)
Severely malformed ear (microtia)
in a Turkish boy who said that he remembered the life of a man who was
fatally wounded on the right side of the head by a shotgun discharged
at close range.
Figure 9 shows fingers almost absent congenitally on one hand
(unilateral brachydactyly) in a child of India who said he remembered
the life of another child who had put his right hand into the blades of
a fodder-chopping machine and lost his fingers. Most cases of brachydactyly
involve only a shortening of the middle phalanges. In the present case
there were no phalangeal bones, and the fingers were represented by mere
stubs. Unilateral brachydactyly is exceedingly rare, and I have not found
a published report of a case, although a colleague (plastic surgeon) has
shown me a photograph of one case that came under his care.
Almost absent fingers (brachydactyly)
on one hand in a boy of India who said he remembered the life of a boy of
another village who had put his hand into the blades of a fodderchopping
machine and had its fingers amputated.
Figure 10 shows congenital absence of the lower right leg (unilateral
hemimelia) in a Burmese girl. She said that she remembered the life of a
girl who was run over by a train. Eyewitnesses said that the train severed
the girl's right leg first, before running over the trunk. Lower hemimelia
is an extremely rare condition, and Frantz and O'Rahilly (1961) found it
in only 12 (4.0%) of 300 cases of all congenital skeletal deficiencies
that they examined.
Figure 10
Congenital absence of lower leg
(unilateral hemimelia) in a girl of Burma who said she remembered the
life of a young woman who was accidentally run over by a train, with her
right leg being severed first.
DISCUSSION:
Because most (but not all) of these cases develop among
persons who believe in reincarnation, we should expect that the informants
for the cases would interpret them as examples according with their belief;
and they usually do.
It is necessary, however, for
scientists to think of alternative explanations. The most obvious
explanation of these cases attributes the birthmark or birth defect on
the child to chance, and the reports of the child's statements and
unusual behavior then become a parental fiction intended to account
for the birthmark (or birth defect) in terms of the culturally accepted
belief in reincarnation.
There are, however, important objections to this explanation.
First, the parents (and other adults concerned in a case) have no need
to invent and narrate details of a previous life in order to explain
their child's lesion.
Believing in reincarnation, as most
of them do, they are nearly always content to attribute the lesion to
some event of a previous life without searching for a particular life
with matching details.
Second, the lives of the deceased persons figuring in the cases were of
uneven quality both as to social status and commendable conduct. A few
of them provided models of heroism or some other enviable quality; but
many of them lived in poverty or were otherwise unexemplary.
Few parents would impose an identification with such persons on their
children.
Third, although in most cases the two families concerned were acquainted
(or even related), I am confident that in at least 13 cases (among 210
carefully examined with regard to this matter) the two families concerned
had never even heard about each other before the case developed.
The subject's family in these cases can have had no information
with which to build up an imaginary previous life which, it later turned out,
closely matched a real one. In another 12
cases the child's parents had heard about the death of the person concerned,
but had no knowledge of the wounds on that person. Limitations of space for
this article oblige me to ask readers to accept my appraisal of these 25
cases for this matter; but in my forthcoming work I give a list of the cases
from which readers can find the detailed reports of the cases and from
reading them judge this important question for themselves.
Fourth, I think I have shown that chance is an
improbable interpretation for the correspondences
in location between
two or more birthmarks on the subject of a case and wounds on a deceased
person.
Persons who reject the explanation of chance combined with a secondarily
confected history may consider other interpretations that include paranormal
processes, but fall short of proposing a life after death. One of these
supposes that the birthmark or birth defect occurs by chance and the
subject then by telepathy learns about a deceased person who had a similar
lesion and develops an identification with that person.
The children
subjects of these cases, however, never show paranormal powers of the
magnitude required to explain the apparent memories in contexts outside
of their seeming memories.
Another explanation, which would leave less to chance in the production
of the child's lesion, attributes it to a maternal impression on the part
of the child's mother. According to this idea, a pregnant woman, having a
knowledge of the deceased person's wounds, might influence a gestating
embryo and fetus so that its form corresponded to the wounds on the
deceased person.
The idea of maternal impressions, popular in preceeding centuries and
up to the first decades of this one, has fallen into disrepute.
Until my own recent article (Stevenson, 1992) there had been no review of
series of cases since 1890 (Dabney, 1890); and cases are rarely published
now (Williams and Pembroke, 1988). Nevertheless, some of the published
cases - old and new - show a remarkable correspondence between an unusual
stimulus in the mind of a pregnant woman and an unusual birthmark or
birth defect in her later-born child.
Also, in an analysis of 113 published
cases I found that the stimulus occurred to the mother in the first trimester
in 80 cases (Stevenson, 1992). The first trimester is well known to be
the one of greatest sensitivity of the embryo/fetus to recognized teratogens,
such as thalidomide (Nowack, 1965) and rubella (Hill, Doll, Galloway,
and Hughes, 1958). Applied to the present cases, however, the theory of
maternal impression has obstacles as great as the normal explanation
appears to have.
First, in the 25 cases mentioned above, the subject's mother, although
she may have heard of the death of the concerned deceased person, had
no knowledge of that person's wounds.
Second, this interpretation supposes
that the mother not only modified the body of her unborn child with her
thoughts, but after the child's birth influenced it to make statements
and show behavior that it otherwise would not have done. No motive for
such conduct can be discerned in most of the mothers (or fathers) of
these subjects.
It is not my purpose to impose any interpretation of these
cases on the readers of this article. Nor would I expect any reader to
reach even a preliminary conclusion from the short summaries of cases that
the brevity of this report entails. Instead, I hope that I have stimulated
readers to examine the detailed reports of many cases that I am now in the
process of publishing (Stevenson, forthcoming).
"Originality
and truth are found only in the details"
(Stendhal, 1926).
ACKNOWLEDGEMENTS:
I am grateful to Drs. Antonia Mills and Emily W. Cook for critical
comments on drafts of this paper. Thanks are also due to the Bernstein
Brothers Parapsychology and Health Foundation for the support of my research.
CONTACT INFORMATION:
Correspondence and requests for reprints should be addressed to:
Ian Stevenson, MD, Division of Personality Studies, Box 152, Health
Sciences Center, University of Virginia, Charlottesville, VA 22908
REFERENCES:
Cockayne, E, A. (1933). Inherited abnormalities of the
skin. London: Oxford University Press.
Cook, E. W., Pasricha, S, Samararatne, G, Win Maung, &
Stevenson, I. (1983). Review and analysis of "unsolved" cases of the
reincarnation type: II. Comparison of features of solved and unsolved
cases, Journal of the American Society for Psychical Research, 77, 1
15-135.
Dabney, W. C. (1890). Maternal impressions. In J. M.
Keating (Ed.), Cyclopaedia of the diseases of children, Vol. 1 , (pp. 1 9
1 -2 1 6). Philadelphia: J. B. Lippincott.
Denaro, S. J. ( 1944). The inheritance of nevi. Journal of
Heredity, 35, 2 1 5- 1 8.
Fatteh, A. (1976). Medicolegal investigation ofgunshor
wounds. Philadelphia: J. B. Lippincott.
Frantz, C. H., & O'Rahilly, R.(1961). Congenital
skeletal limb deficiencies. Journal ofBone and Joins Surgerq: 43-A,
1202-24.
Gordon, I., & Shapiro, H. A. (1982). Forensic
medicine: A guide to principles. (2nd ed.) London: Churchill
Livingstone.
Hill, A, B,, Doll, R,, Galloway, T. M., & Hughes,
J.P.W. (1958). Virus diseases in pregnancy and congenital defects. British
Journal of Preventive and Social Medicine, 12, 1-7.
Maruri, C. A. (1961). La herencia en dermarologia. (2nd
ed.) Santander: Aldus, S.A. Artes Graficas.
Mills, A. (1989). A replication study: Three cases of
children in northern India who are said to remember a previous life.
Journal of Scientific Exploration, 3, 133-184.
Nelson, K., & Holmes, L. B. (1989). Malformations due
to presumed spontaneous mutations in newborn infants. New England Journal
of Medicine, 320, 19-23.
Nowack, E, (1965). Die sensible Phase bei der Thalidomid-
Embryopathie. Humangenetik, I, 516-36.
Pack, G. T., & Davis, J. (1956). Moles. New York Stare
Journal ofMedicine, 56, 3498-3506.
Pack, G. T., Lenson, N. & Gerber, D. M. (1952).
Regional distribution of moles and melanomas. AMA Archives ofSurgery. 65,
862-70.
Smith, D. W. (1982). Recognizable patterns of human
malformation. (3rd ed.) Philadelphia: W. B·Saunders.
Spalteholz. W· (1943). Hand atlas of human anatomy.
Translated by L. E Barker. 7th English ed. Philadelphia: J. B. Lippincott.
Stevenson, I. (1975). Cases of the reincarnation type. I.
Ten cases in India. CharlottesviIle: University Press of Virginia.
Stevenson, I. (1983). American children who claim to
remember previous lives. Journal of Nervous and Mental Disease, 17 1,
742-748.
Stevenson, I. (1987). Children who remember previous
lives. Charlottesville: University Press of Virginia.
Stevenson, I. ( 1990). Phobias in children who claim to
remember previous lives. Journal of Scientific Exploration, 4,
243-254.
Stevenson, I. (1992). A new look at maternal impressions:
An analysis of 50 published cases and reports of two recent examples.
Journal of Scientific Exploration, 6, 353-373.
Stevenson, I. (Forthcoming). Birthmarks and birth defects:
A contribution to their etiology.
Williams, H. C., & Pembroke, A. C. (1988). Naevus of
Jamaica. Lancer, 11, 915.
Wilson, J. G. (1973). Environment and birth defects. New
York: Academic Press.





 Past Lives and Birthmarks
Past Lives and Birthmarks ABSTRACT:
Almost nothing is known about why pigmented birthmarks
(moles or nevi) occur in particular locations of the skin. The causes of
most birth defects are also unknown. About 35% of children who claim to
remember previous lives have birthmarks and/or birth defects that they (or
adult informants) attribute to wounds on a person whose life the child
remembers. The cases of 210 such children have been investigated.
ABSTRACT:
Almost nothing is known about why pigmented birthmarks
(moles or nevi) occur in particular locations of the skin. The causes of
most birth defects are also unknown. About 35% of children who claim to
remember previous lives have birthmarks and/or birth defects that they (or
adult informants) attribute to wounds on a person whose life the child
remembers. The cases of 210 such children have been investigated. Figure 1
Figure 1
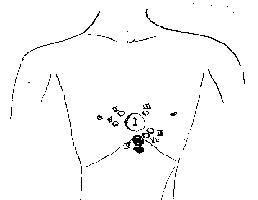 Figure 2
Figure 2
 Figure 3
Figure 3
 Figure 4
Figure 4
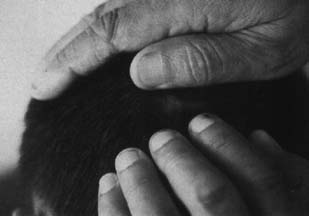 Figure 5
Figure 5
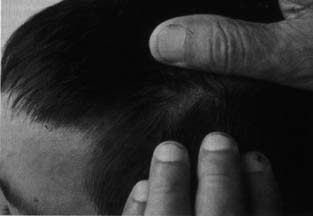 Figure 6
Figure 6
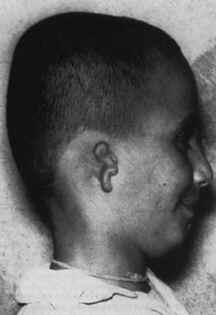

 Figure 10
Figure 10